

Abstract

Introduction
Thrombocytopenia is a common complication after allogeneic hematopoietic stem cell transplantation (allo-SCT). Underlying mechanisms are poorly known and usually multifactorial. Its treatment is not well defined, mostly based in platelet transfusion. Thus, is important to identify new strategies to manage this important post-SCT complication. Romiplostim and Eltrombopag are currently available thrombopoietin receptor agonists (TPO-RAs) that stimulate platelet production. Some studies with very small number of cases have reported their potential efficacy in the allo-SCT setting. For this reason, the aim of our study is to analyze the efficacy and safety of TPO-RAs for severe and persistent thrombocytopenia after allo-SCT.
Patients and methods
We performed a retrospective multicenter study including patients from centers of GETH with prolonged isolated thrombocytopenia (PT) or secondary failure of platelet recovery (SFPR) after allo-SCT. PT was defined as the engraftment of all peripheral blood cell lines but with platelet count ≤20000/µL for 7 consecutive days or requirement of transfusion for more than 60 days after allo-SCT. SFPR was defined as a decline of platelet counts to ≤20000/µL for 7 consecutive days or requirement of transfusion after achievement platelets ≥50000/µL without transfusion for 7 days post-SCT. The primary endpoint was platelet recovery to ≥50000/µL.
Results
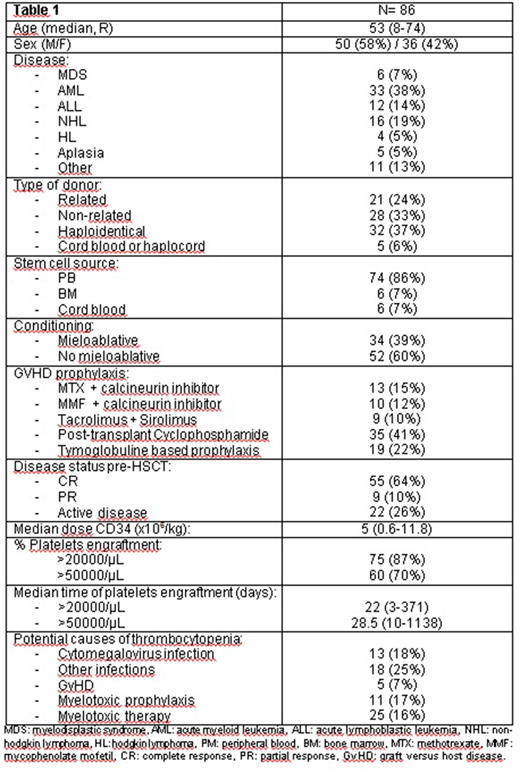
Eighty-six patients with thrombocytopenia after allo-SCT were included. The characteristic of the patients, are summarized in table 1. Sixteen (19%) of the patients had PT and 71 (82%) SFPR. TPO-RA was started at a median time of 127 days (27-1177) after allo-SCT (41% Romiplostim / 59% Eltrombopag). Median initial and maximum administered doses were 50 mg/daily (25-150) and 75 (25-150) for Eltrombopag and 1 µg/kg (1-7) and 5 (1-10) for Romiplostin, respectively. Eighteen patients (21%) were previously treated with cell infusion (67% mesenchymal cells and 33% CD34+ boost). Median platelet count before TPO-RA onset was 14000/µL (1000-57000). Platelet recovery to ≥50000/µL was 60% and the response was achieved at a median time of 56 days (2-247). Responses were similar considering all potential causes of thrombocytopenia evaluated. 81% of the patients had decrease number of megakaryocytes prior to treatment showing a worse response to therapy: median time to ≥20000/µL platelets 43 days versus 28 days (p=0.011), with also a lower rate of platelet recovery to ≥50000/µL (62% versus 85% if normal megakaryocytes). In patients treated with Eltrombopag, 27% had neutropenia <1000/µL and 74% achieved >1000/µL after therapy. The median treatment duration was 62 days (7-700) and 62% discontinued TPO-Ra maintaining response. Grade 3-4 adverse events (hepatic and asthenia) were observed in only 2% of the cases. At last follow up with a median of 10 months (1-59), 72% of the patients maintained the response and 61 (71%) were alive. Death rate was significantly lower in responder-patients to TPO-RAs, 15% versus 53% in non-responders (p<0.001). Causes of death were disease progression (28%), infections (48%), graft versus host disease (GvHD) (16%) and others (8%).
Conclusion
To our knowledge this is the biggest series analyzing the use of TPO-Ra after allo-SCT. Our results support the efficacy and safety in this new setting with responses around 60% and a low number of side effects. Additional studies to identify predictors of response are needed.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal